Frozen Shoulder and Menopause: Why Your Shoulder Might Be Shouting at You
Do you ever have mornings where you get out of bed and feel like a 90-year-old woman?
I do.
Some mornings I honestly feel like the Tin Man from The Wizard of Oz, creaking my way into the day until everything finally starts moving.
And if you’re nodding along, you are definitely not on your own.
One of the things no one really warns us about in menopause is how much it can affect our muscles, joints, bones, tendons and connective tissue. We hear plenty about hot flushes, sleep, mood and periods. But the creaky knees, the stiff hips, the sore feet, or the random aches that seem to move around your body like they’re on tour? Not so much.
This is now being discussed as the Musculoskeletal Syndrome of Menopause, or MSM.
I know. Another menopause acronym. As if we didn’t have enough to be getting on with.
But this one is useful because it gives language to something women have been describing for years: why does my body suddenly feel like it needs an extended warranty?
MSM refers to the changes many women experience in muscles, joints, bones, tendons and connective tissue during perimenopause and postmenopause.
It can include:
joint aches and pains
stiffness, especially in the morning
loss of muscle mass
changes in bone density
tendon issues
plantar fasciitis
worsening arthritis symptoms
increased fracture risk
and yes, frozen shoulder
And frozen shoulder is the one I want to focus on here, because it is one of those symptoms that can really catch women off guard.
One day you’re brushing your hair, fastening your bra, lifting a bag, reaching for the remote, or trying to put a saucepan back into the cupboard. The next minute your shoulder has staged a full protest. No warning, no consultation, no memo. Just pain, stiffness and that lovely moment where a basic everyday movement has somehow turned into a round of Ninja Warrior.
So let’s talk about frozen shoulder. And yes, it is as delightful as it sounds.

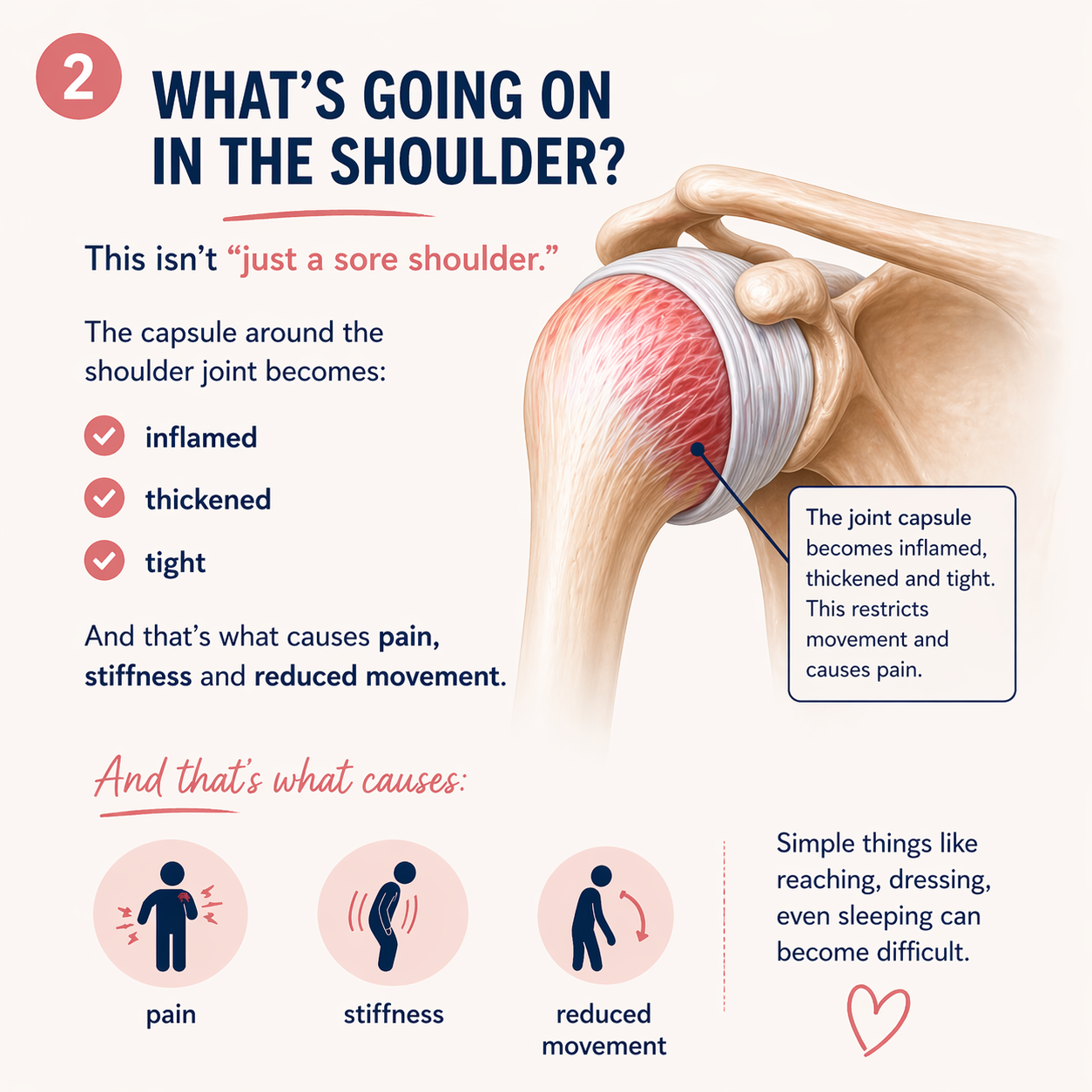
What is frozen shoulder?
Frozen shoulder, also known as adhesive capsulitis, happens when the shoulder becomes painful, stiff and increasingly difficult to move.
It can creep in slowly, and often the first thing women notice is that something just feels “off”.
You may find it harder to:
reach overhead
fasten your bra
brush or wash your hair
lift something into a cupboard
sleep on that side
get dressed without wincing
reach behind you in the car
And because menopause likes to keep things interesting, the pain can also wake you at night, as if sleep wasn’t already under enough pressure.
The shoulder is one of those parts of the body we completely underestimate until it stops working properly. We use it constantly for strength, balance, lifting, reaching, dressing, driving and doing about fifty things before breakfast, so when it becomes stiff or painful, it can affect everything.
Why does frozen shoulder happen?
The annoying answer is that we don’t always know.
Frozen shoulder can happen without an obvious cause, but we do know there are certain factors that can increase the risk.
These include:
diabetes
thyroid conditions, both underactive and overactive
previous shoulder injury or surgery
long periods where the shoulder has not been moving much
heart disease
other shoulder issues such as rotator cuff problems
age, particularly between 40 and 60
being female
And then, of course, we have menopause.
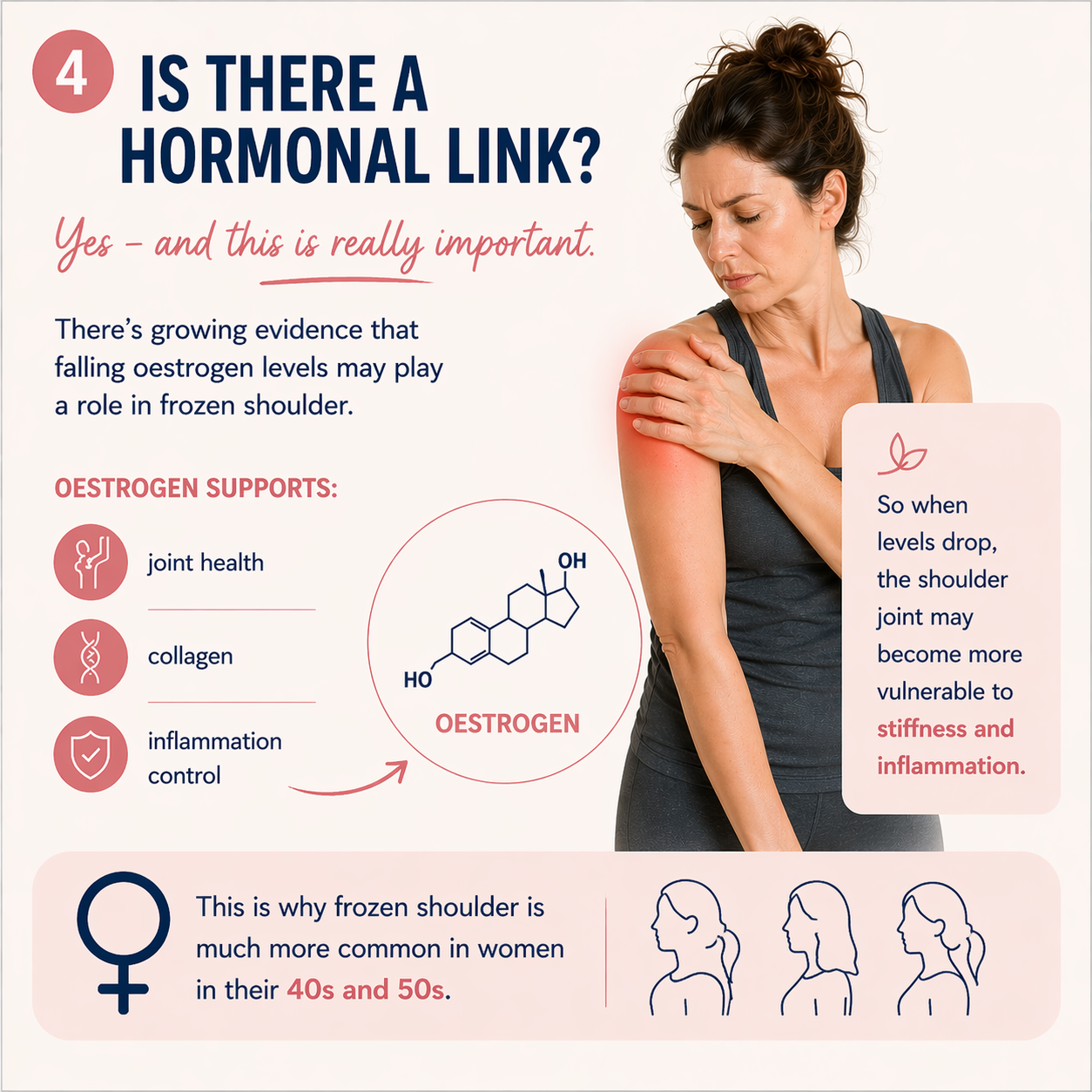
What is the link between frozen shoulder and menopause?
Oestrogen is not just about periods, hot flushes and whether we can remember why we walked into a room.
This superstar hormone has receptors throughout the body, including in muscles, joints, tendons, ligaments and connective tissue.
It plays a role in inflammation, tissue repair, collagen, cartilage, joint health and how the body maintains strength and flexibility. Oestrogen also supports the cells that help maintain cartilage, the smooth tissue that cushions our joints. It has anti-inflammatory effects too, so when oestrogen fluctuates and then declines, some women may notice more aches, stiffness, tendon issues and joint pain.
And this is where frozen shoulder may fit into the bigger musculoskeletal picture.
Now, we do need to be careful here. We can’t say menopause “causes” frozen shoulder in every case. It’s usually more complex than that. Ageing, previous injury, activity levels, inflammatory conditions, sleep, stress, thyroid health, blood sugar and general health all matter too.
But menopause can absolutely be part of the story, and for many women, simply knowing that is a relief.
You’re not imagining it. You’re not suddenly “getting old overnight”. Your body is changing, and it may need a different level of support now.
The stages of frozen shoulder
Frozen shoulder often moves through stages, although not everyone fits neatly into the textbook version.
1. The painful or “freezing” stage
This is where pain tends to build. Movement becomes harder and sleep may be affected. Lovely.
2. The stiff or “frozen” stage
The pain may ease a bit, but the shoulder can feel very restricted. This is often when everyday tasks become really frustrating.
3. The thawing stage
Movement gradually starts to return.
And this is the bit I really want you to hear: frozen shoulder can be slow. Really slow. It can take months, and for some people longer, to fully settle. But the good news is that most people do improve.
It may require patience, consistency and the right support, but this is not your shoulder being broken forever. It is a condition that can heal.

What can help frozen shoulder?
The first thing I would say is please don’t try to “push through” severe shoulder pain. I know we’re all inclined to think, I’ll just stretch it out, but with frozen shoulder, forcing movement aggressively can make things angrier.
A physiotherapist is often the mothership of recovery here. They can assess what is actually going on and give you exercises that are right for your stage of recovery, because what helps at one stage may be too much at another.
Some common supportive approaches include:
Physiotherapy: This is usually one of the key supports. A good physio can help with mobility, strength and function, while making sure you’re not overdoing it.
Gentle movement: The word here is gentle. Not yanking, not forcing, and not deciding you’ll “sort it out” with one heroic stretch. Think small, consistent movements such as pendulum swings, wall walks with your fingers, gentle external rotation stretches, towel-assisted stretches or shoulder blade squeezes. Please get guidance, especially if pain is significant.
Pain management: If pain is affecting your sleep or your ability to function, speak to your GP or pharmacist. You do not get a medal for suffering through pain.
Heat or cold: Some people find heat helpful for stiffness, while others prefer cold if the shoulder feels inflamed or painful. It can be a bit of trial and error.
Strength work, at the right time: Strength training is brilliant for us in midlife and beyond, but timing matters. If your shoulder is in a very painful phase, you may need to focus first on calming things down and restoring gentle movement. Then strength can be built back in gradually.
Magnesium and omega-3: These won’t “cure” frozen shoulder, but they may support muscle function and inflammation as part of your overall toolkit. I always come back to the full picture: nutrition, sleep, stress, movement, hormones, and medical support where needed. It is rarely one thing.
Can HRT help frozen shoulder?
This is an area that is getting more attention.
Some emerging research suggests that women using HRT may have a lower risk of frozen shoulder, possibly because of oestrogen’s role in reducing inflammation and supporting connective tissue health.
But, as with so many aspects of menopause, more research is needed.
HRT is not a frozen shoulder treatment on its own, and it won’t be suitable or wanted by everyone. But if you’re in menopause and struggling with frozen shoulder, joint pain, tendon issues or other musculoskeletal symptoms, it is absolutely worth having a proper conversation with your doctor about your full picture.
Not a rushed “you’re just getting older” conversation. A proper one.
What about dry needling?
Some people find dry needling helpful, particularly where muscles around the shoulder and neck are going into spasm or holding tension.
I’ve had dry needling myself recently for an IT band issue and honestly, the relief was unbelievable.
That said, it needs to be done by a properly qualified practitioner, and it’s not for everyone. Again, the boring but important message: get assessed properly.
Frozen shoulder, thyroid issues and diabetes
This is an important one.
Frozen shoulder is more common in people with diabetes and thyroid conditions, so if you are dealing with frozen shoulder, it is worth having these on your radar.
This is particularly important if you also have symptoms such as:
fatigue
weight changes
changes in temperature tolerance
palpitations
constipation
thirst
changes in urination
energy crashes
I’m not saying panic. I am saying be proactive. Ask your doctor whether thyroid function and blood sugar markers need to be checked, especially if this hasn’t been done recently.
What about stress and frozen shoulder?
I want to be careful with this one.
You may hear people say frozen shoulder is linked to emotional trauma, grief or “carrying burdens”. I don’t like when physical pain is explained away as purely emotional. That can feel very dismissive, especially when you’re in real pain.
But we also know that stress, grief and emotional load can affect the body. Pain and stress can feed into each other. If you are not sleeping, if your nervous system is on high alert, if your body is tense all the time, it can make pain harder to manage.
So yes, support the emotional side too. That might be rest, counselling, journaling, mindfulness, breathwork, talking to a friend, or simply giving yourself permission to say: this is hard, and I need support.
That is not weakness. That is wisdom.
Final thoughts
Frozen shoulder can be incredibly frustrating. It can make you feel older than you are, and it can disrupt sleep, movement, exercise, work and the simple daily things we usually take for granted.
But it can improve. It takes patience, consistency, the right support, and sometimes far longer than we would like.
If your shoulder is painful, stiff or your range of movement has changed, please don’t ignore it and hope it magically disappears while you wrestle yourself into a jacket every morning. Get it checked. See a physio. Talk to your doctor. Look at the full picture: hormones, thyroid, blood sugar, inflammation, strength, sleep and stress.
And most importantly, be kind to yourself. You are not falling apart. Your body is asking for support in a new way.
Listen to it.